
Introduction
Many UK adults don’t know their cholesterol numbers, and even fewer understand what those numbers actually mean for their long-term health. High cholesterol doesn’t cause symptoms. It doesn’t make you feel unwell. It quietly damages arteries for decades before producing the heart attack, stroke, or vascular event that finally makes it visible.
This invisible nature is exactly why cholesterol management is one of the most under-treated areas in UK health. NHS GPs are stretched thin. NICE guidance changed substantially in December 2023 with the publication of NG238, but many patients are still being managed against older frameworks. New medications like inclisiran (a twice-yearly injection) have transformed treatment options for high-risk patients, yet most patients have never heard of them.
This guide explains how private cholesterol treatment works in the UK in 2026, what the current evidence actually says, what realistic costs look like, and how to decide whether private care is the right pathway for your situation. It is written by a UK-registered pharmacist and aligns with NICE NG238 (the current UK cholesterol management guideline), which was updated in December 2023.
What Is High Cholesterol, Really?
Cholesterol is a waxy substance that travels through your bloodstream attached to proteins called lipoproteins. There are several types, but for clinical purposes, three numbers matter most:
LDL cholesterol (“bad” cholesterol): Low-density lipoprotein. This is the type that deposits in artery walls, causing atherosclerosis. Lowering LDL is the central goal of most cholesterol treatment.
HDL cholesterol (“good” cholesterol): High-density lipoprotein. This helps remove cholesterol from the arteries. Higher HDL is generally protective, though raising HDL with medication hasn’t been shown to reduce cardiovascular events.
Non-HDL cholesterol: Total cholesterol minus HDL. This captures all the “bad” lipoproteins together (LDL plus other harmful fractions). NICE NG238 now prefers non-HDL as the primary target because it doesn’t require fasting and correlates more closely with cardiovascular outcomes.
In addition, triglyceride levels often rise alongside cholesterol, particularly in patients with insulin resistance, type 2 diabetes, or metabolic syndrome.
The relationship between cholesterol and heart disease has been studied more thoroughly than almost any other intervention in medicine. The evidence base spans 30+ years of large randomised controlled trials and millions of patient-years of follow-up. The conclusion is consistent: lowering LDL cholesterol reduces the risk of heart attacks, strokes, and cardiovascular death.
NICE NG238: The Current UK Cholesterol Framework
NICE replaced the older CG181 guideline with NG238 in December 2023. The changes are meaningful and not yet fully reflected in routine NHS practice for many patients.
Key Updates In NG238
1. Non-HDL cholesterol is now preferred over LDL. Total cholesterol minus HDL. Easier to measure (no fasting required), better correlation with outcomes.
2. Risk assessment via QRISK3. QRISK3 estimates 10-year cardiovascular risk based on age, sex, ethnicity, blood pressure, cholesterol, smoking status, family history, and several comorbidities. A QRISK3 score ≥ 10% triggers consideration of statin therapy for primary prevention.
3. Primary prevention treatment goal. For patients without established cardiovascular disease (primary prevention), NICE NG238 recommends targeting a ≥40% reduction in non-HDL cholesterol from baseline as the primary therapeutic goal. The starting drug is atorvastatin 20mg for most adults requiring statin therapy for primary prevention.
4. Secondary prevention targets. For patients with established cardiovascular disease, NICE recommends targeting:
- LDL ≤2.0 mmol/L, OR
- Non-HDL ≤2.6 mmol/L
5. Atorvastatin 80mg as the secondary prevention default. For patients post-MI, post-stroke, or with established CVD, atorvastatin 80mg is the standard starting point.
5. Newer agents integrated. NG238 includes ezetimibe, bempedoic acid, PCSK9 inhibitors (evolocumab, alirocumab), inclisiran, bile acid sequestrants, and fibrates (in specific scenarios) as treatment options within a stepped pathway.
Calculating Your Non-HDL Cholesterol
The non-HDL calculation is genuinely simple and worth knowing if you’re tracking your own cholesterol numbers between blood tests.
Non-HDL cholesterol = Total cholesterol − HDL cholesterol
(All values in mmol/L)
Example: Total cholesterol 5.2 − HDL 1.3 = Non-HDL 3.9 mmol/L
Unlike LDL calculation (which traditionally required the Friedewald equation and a fasting sample), non-HDL can be calculated from any standard cholesterol blood test, fasted or non-fasted. This is one of the practical reasons NICE NG238 moved to non-HDL as the preferred primary marker.
Reference Lipid Levels For Context
These are general reference ranges, not treatment targets. NICE targets in primary prevention are based on percentage reduction from baseline (≥40% non-HDL reduction), and in secondary prevention on absolute thresholds.
| Marker | General Reference (mmol/L) | Secondary prevention target (NICE NG28) |
|---|---|---|
| Total Cholesterol | <5.0 | – |
| LDL Cholesterol | <3.0 | ≤2.0 |
| Non-HDL Cholesterol | <4.0 | ≤2.6 |
| HDL cholesterol | >1.0 (men), > 1.2(women) | – |
| Triglycerides (Fasting) | <1.7 | – |
| Total cholesterol : HDL ratio | < 4.0 | – |
| – | – |
Important context: HDL and triglycerides are descriptive markers in NICE NG238, not direct treatment targets. Very low HDL or very high triglycerides do prompt further investigation but are not directly treated with medication for cardiovascular prevention purposes (except severe hypertriglyceridaemia, which is treated to prevent pancreatitis rather than cardiovascular events).
The NICE NG238 Treatment Pathway
The cholesterol treatment pathway splits early into two distinct branches depending on whether you’re managing primary prevention (no existing cardiovascular disease) or secondary prevention (established cardiovascular disease such as a previous heart attack, stroke, or angina). After Step 2, the two pathways differ: primary prevention patients start at a lower statin dose with room to escalate, whereas secondary prevention patients begin at the maximum atorvastatin dose.
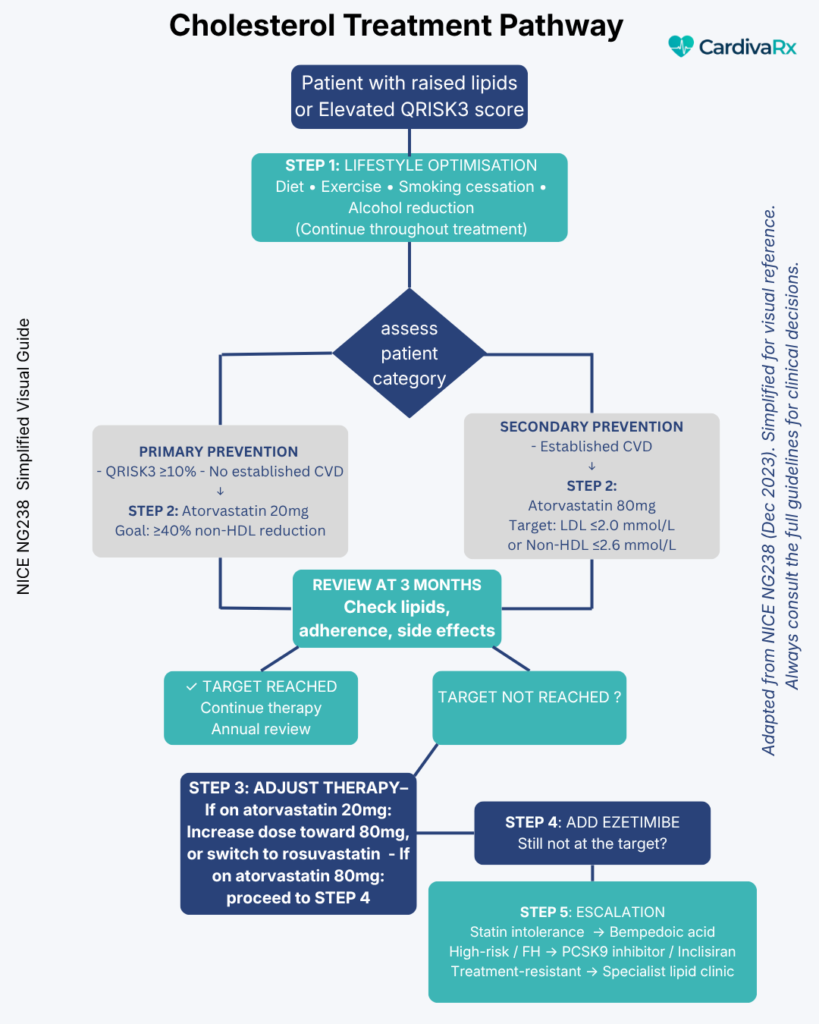
Important Clinical Note On The Branched Pathway
The pathway diverges at Step 3 because secondary-prevention patients begin treatment with atorvastatin 80mg, already the highest available statin dose. There is no higher-intensity statin to switch to. For these patients, “optimising the statin” is not an option because they are already at maximum therapy.
This is why:
- Primary prevention patients who don’t reach the ≥40% non-HDL reduction goal at Step 2 (atorvastatin 20mg) proceed to Step 3 (statin optimisation—increasing the dose toward 80mg or switching to rosuvastatin) before adding ezetimibe at Step 4.
- Secondary prevention patients who don’t reach LDL ≤2.0 mmol/L or non-HDL ≤2.6 mmol/L at Step 2 (atorvastatin 80mg) skip directly to Step 4 (add ezetimibe) because dose escalation is no longer possible.
Before assuming a patient hasn’t responded to therapy, NICE emphasises checking adherence and modifiable factors (smoking, weight, alcohol intake, drug interactions); many apparent “treatment failures” resolve with these reviews rather than escalation.
The full NICE NG238 guideline includes additional specific considerations for type 2 diabetes, chronic kidney disease, familial hypercholesterolaemia, and pregnancy. For complex cases, a referral to a specialist lipid clinic remains appropriate.
NHS Cholesterol Treatment vs Private Cholesterol Treatment
For most UK patients with raised cholesterol, the NHS pathway works as designed. It identifies risk through QRISK3, offers lifestyle advice, and prescribes statins where indicated. For straightforward cases, this is appropriate care.
Private cholesterol treatment is available for patients for whom the NHS pathway doesn’t fit well. Three common situations:
When NHS Cholesterol Care Works Well
- Newly identified high cholesterol with no urgency
- Straightforward statin initiation with no complications
- Stable, well-controlled patients on long-term therapy
- Patients who don’t mind 8-12 week waits between reviews
When Private Cholesterol Treatment Adds Value
1. Statin intolerance. Patients who experience side effects on multiple statins often hit a wall in NHS practice. GPs may not have time to systematically work through alternative statins, ezetimibe combinations, bempedoic acid, or newer agents. Private specialist input can navigate this complexity.
2. Inadequate cholesterol control on standard therapy. Patients who don’t reach NICE targets despite full-dose statin may benefit from add-on therapy (ezetimibe) or escalation to newer agents (bempedoic acid, PCSK9 inhibitors, inclisiran). The NHS pathway to these agents typically requires lipid clinic referral, and waits of 6-12+ months are common.
3. Comprehensive cardio-metabolic management. Cholesterol rarely exists in isolation. Patients with elevated cholesterol often also have elevated blood pressure, elevated blood glucose, and increased weight. Treating each separately through different NHS pathways misses the integrated picture. Private cardio-metabolic services address all three together.
Comparison Table: NHS vs Private Cholesterol Treatment
| Feature | NHS Cholesterol Treatment | Private Cholesterol Treatment |
|---|---|---|
| Cost | Free | Self-pay (typically £30–£100 initial consultation, £10–£40/month medication for online pharmacist IP services; private GPs and specialists cost more) |
| Initial consultation length | 10 minutes (GP) | 20–30 minutes |
| Time to treatment initiation | 4-8 weeks typical | 1-2 weeks |
| Cholesterol blood tests | ✓ | ✓ (private lab if preferred) |
| QRISK3 risk assessment | ✓ | ✓ |
| Lifestyle counselling | Limited (brief mention) | Structured discussion |
| Standard statin prescribing | ✓ | ✓ |
| statin intolerance management | Limited (often “try another GP appointment”) | Systematic alternative pathway |
| Ezetimibe/ combination therapy | ✓ (often delayed) | ✓ (immediate if indicated) |
| Bempedoic acid access | Limited (often specialist referral required) | ✓ |
| PCSK9 inhibitor / inclisiran access | Specialist lipid clinic referral (6-12+ months wait) | Faster specialist referral coordination |
| Same prescriber every visit | ✗ | ✓ |
| Cardio-metabolic integration (BP + glucose + lipids) | ✗ | ✓ |
| Review schedule | Annual typical | Quarterly or as needed |
The strategic point is that the NHS works well for the straightforward case. Private specialist services exist for cases where complexity, intolerance, or inadequate control creates a gap.
Why Patients Pay For Private Cholesterol Treatment
Five common reasons patients move to private care:
1. Statin side effects that the NHS didn’t resolve. Patients who’ve tried two statins, experienced muscle aches or fatigue on both, and been told “let’s just try another one” or “we can stop the statin then.” A systematic approach that works through atorvastatin, rosuvastatin, simvastatin, pravastatin, alternative dosing schedules, and the adjunct ezetimibe often resolves intolerance that GP appointments don’t have time to investigate.
2. Not reaching cholesterol targets. Patients with established CVD whose LDL remains above 2.0 mmol/L or non-HDL above 2.6 mmol/L despite full-dose statin. NICE NG238 indicates step-up therapy in this scenario, but NHS routes can be slow. Private specialist input can accelerate access to ezetimibe combinations or newer agents.
3. Newer treatment access. Inclisiran (twice-yearly injection) is approved by NICE for secondary prevention in eligible patients but remains underutilised in NHS practice. Bempedoic acid for genuine statin intolerance. PCSK9 inhibitors for very high-risk patients. Private specialists can navigate access faster.
4. Cardio-metabolic context. Patients with raised cholesterol, blood pressure, and blood glucose are treated by different NHS clinicians on different schedules, with no integrated overview. Private cardiometabolic services consolidate this into a single specialist relationship.
5. Time, depth, and continuity. 20-30 minute consultations vs 10-minute GP slots. The same prescriber every visit, building knowledge of the patient’s specific clinical picture over time. Detailed explanations of medications, side effects, and alternatives.
The cost of private cholesterol treatment is real. So is the cost of suboptimal cholesterol management measured in cardiovascular events that occur decades later. For many patients, the comparison isn’t private care vs free care; it’s structured proactive management vs reactive episodic care.
Modern Cholesterol Medications Explained
Understanding the medications available helps patients participate in their own treatment decisions.
Statins
The foundation of cholesterol management since the 1990s. They work by inhibiting HMG-CoA reductase, an enzyme involved in liver cholesterol production. This reduces LDL by 25-50% depending on statin and dose.
UK first-line statins:
- Atorvastatin — Most commonly prescribed. Effective across the dose range (10mg to 80mg). Once-daily, any time. Atorvastatin 20mg is the NICE NG238 primary prevention starting dose; 80mg is the secondary prevention starting dose.
- Rosuvastatin — Slightly more potent at equivalent doses. Useful when atorvastatin is not tolerated.
- Simvastatin — Historic standard, now used less due to drug interaction issues.
- Pravastatin — Lower potency but useful in patients sensitive to other statins.
- Fluvastatin — Lower potency, less commonly used.
Statin Intensity: How Much LDL Reduction To Expect
NICE classifies statins by their LDL-lowering potency. High-intensity statins (≥40% LDL reduction) are NICE’s preferred choice for both primary and secondary prevention. The percentage reductions below are based on the BNF and standard clinical references.
| Statin and dose | Approximate LDL reduction | NICE classification |
|---|---|---|
| Atorvastatin 80mg | 55% | High intensity |
| Atorvastatin 40mg | 49% | HIgh intensity |
| Atorvastatin 20mg | 43% | High intensity |
| Atorvastatin 10mg | 37% | Medium intensity |
| Rosuvastatin 40mg | 53% | High intensity |
| Rosuvastatin 20mg | 48% | High intensity |
| Rosuvastatin 10mg | 43% | High intensity |
| Rosuvastatin 5mg | 38% | Medium intensity |
| Simvastatin 80mg | 42% | High intensity (not Recommended – myopathy risk |
| Simvastsatin 40mg | 37% | Medium intensity |
| Simvastatin 20mg | 32% | medium intensity |
| Simvastatin 10mg | 27% | Low intensity |
| Pravastatin 40mg | 29% | Low intensity |
| Pravastatin 20mg | 24% | Low intensity |
| Pravastatin 10mg | 20% | Low intensity |
| Fluvastatin 80mg | 33% | Medium intensity |
| Fluvastatin 40mg | 23% | Low intensity |
| Fluvastsain 20mg | 17% | Low intensity |
The clinical implication: when NICE NG238 recommends a high-intensity statin, it specifically means atorvastatin 20mg or above, or rosuvastatin 10mg or above. Lower-intensity options exist but are reserved for patients who can’t tolerate higher doses, who have specific contraindications, or who need cautious dose escalation.
Statin Dosing In Patients Of Asian Ancestry
Patients of Asian ancestry require modified rosuvastatin dosing. This isn’t about cultural identity, it’s about pharmacokinetics. Genetic variants in the transporters that move rosuvastatin out of liver cells (SLCO1B1 and ABCG2) are more common in Asian populations, leading to higher blood concentrations of the drug at equivalent doses.
The UK Summary of Product Characteristics specifies:
- Recommended starting dose: 5mg daily (rather than the usual 10mg)
- The maximum dose is generally 20mg daily; increases above this should only be considered after careful risk-benefit assessment
- 40mg dose is contraindicated in patients of Asian ancestry
This applies specifically to rosuvastatin. Atorvastatin does not require dose adjustment based on Asian ancestry; patients can use the standard dosing range.
The clinical practice implication: when a patient of Asian ancestry needs a high-intensity statin, atorvastatin 20mg or above is often the more straightforward choice. Rosuvastatin remains an option but requires the careful starting-dose and maximum-dose adjustments noted above.
Statin Drug Interactions: What To Know
Statins have well-characterised drug interactions worth understanding. The clinical priority is preventing myopathy (muscle damage), which becomes more likely when statin blood concentrations rise above intended levels due to interacting medications.
Medications that increase statin levels (myopathy risk):
| Interacting medication | Mechanism | Clinical implication |
|---|---|---|
| Clarithromycin and erythromycin | CYP3A4 inhibition | Avoid combination; use an alternative antibiotic or temporarily hold statin |
| Itraconazole, ketoconazole, fluconazole | CYP3A4 inhibition | Avoid or significantly reduce statin dose |
| Diltiazem, verapamil | CYP3A4 inhibition | Lower atorvastatin/simvastatin max doses apply (see below) |
| Amiodarone | CYP3A4 inhibition | Simvastatin max 20mg with amiodarone |
| Ciclosporin | CYP3A4 inhibition | Use specific statins with dose adjustment under specialist advice |
| HIV protease inhibitors (e.g ritonavir) | CYP3A4 inhibition | Specialist input required |
| Gemfibrozil (a fibrate) | inhibits enzymes such as (OATP1B1) | Combination contraindicated for most statins |
| Grapefruit juice | CYP3A4 inhibition | Avoid. Significant interaction with simvastatin and atorvastatin |
| Colchicine | Additive myopathy effect | Caution and monitor for muscle symptoms |
Other significant interactions:
- Warfarin: Statins can modestly enhance the anticoagulant effect. INR may need monitoring when starting or stopping a statin in patients on warfarin.
- Other fibrates (fenofibrate, bezafibrate): Coadministration with statins increases the risk of myopathy. NICE NG238 recommends avoiding this combination for cardiovascular prevention.
Statins with fewer interaction concerns:
Rosuvastatin and pravastatin are less dependent on CYP3A4 metabolism, making them useful in patients with significant polypharmacy where CYP3A4 interactions are problematic. This is one reason rosuvastatin is sometimes preferred in older patients on multiple medications, with fewer interaction concerns at standard doses.
If you’re starting or changing a statin and take other prescription medications, your prescriber should review the full interaction profile. This is also a meaningful reason to use a specialist cardio-metabolic service where the consultation has time to systematically review medications, rather than a brief GP appointment that may not catch subtle interactions.
Where Cardio-Metabolic Conditions Overlap: Why Integrated Care Matters
One of the most clinically important UK drug interactions sits exactly at the intersection of hypertension and cholesterol management. Patients on amlodipine, one of the most commonly prescribed first-line UK antihypertensives, face a specific interaction with simvastatin that’s been under-recognised in routine practice.
The amlodipine-simvastatin interaction:
Amlodipine inhibits CYP3A4, the enzyme that breaks down simvastatin. When the two are combined, simvastatin blood levels rise; research suggests effective exposure equivalent to 80mg of simvastatin when only 40mg is prescribed. This increases the risk of myopathy and rhabdomyolysis.
The MHRA Drug Safety Update (August 2012) sets the rule:
- Maximum simvastatin dose with amlodipine: 20mg daily
- Simvastatin 40mg or 80mg with amlodipine is off-label and not recommended
The same 20mg maximum applies when simvastatin is combined with:
- Verapamil
- Diltiazem
- Amiodarone
These are all CYP3A4 inhibitors used in cardiovascular care.
Practical management options:
When a patient on amlodipine needs higher-intensity cholesterol lowering than simvastatin 20mg provides:
- Switch to atorvastatin (much lower interaction risk with amlodipine and other CYP3A4 inhibitors)
- Switch to rosuvastatin (metabolised differently from CYP3A4, minimal interaction concern)
- Reduce simvastatin to 20mg and add ezetimibe if additional lowering is needed
The cleanest solution for most patients is option 1, atorvastatin, which works at the standard dosing range alongside amlodipine without interaction concerns. This is one reason atorvastatin has largely replaced simvastatin as the UK default in patients with combined hypertension and dyslipidaemia.
Why this matters for integrated care:
This is a clinically real example of why managing hypertension, cholesterol, and other cardio-metabolic conditions together makes sense. A patient seeing a hypertension GP for amlodipine and a separate cholesterol pathway for simvastatin may have both prescriptions optimised independently, but the combination creates a risk neither prescriber may have flagged.
Real-world UK data show that this interaction is still regularly missed in NHS prescribing audits. Specialist cardio-metabolic services that manage all three conditions together, blood pressure, glucose, and lipids, naturally identify these intersections at the point of prescribing rather than relying on separate clinicians to coordinate.
For more on UK hypertension treatment options, including amlodipine, see our complete guide to private hypertension treatment in the UK.
The evidence base for statins is overwhelming. Trials from 4S (1994) through HPS (2002), JUPITER (2008), and the Cholesterol Treatment Trialists’ meta-analyses of 170,000+ patients all show consistent benefit. Every 1 mmol/L reduction in LDL is associated with approximately a 22% reduction in the risk of major cardiovascular events.
Ezetimibe
Inhibits cholesterol absorption in the small intestine. Provides additional LDL reduction of 15-25% when added to a statin. The IMPROVE-IT trial (2015) established that adding ezetimibe to statin reduces cardiovascular events further than statin alone.
Often used when statins alone don’t achieve the target, or when statin dose escalation is limited by side effects.
Bempedoic Acid
A relatively new option (UK approval 2020). Works on the same cholesterol synthesis pathway as statins, but at a different enzymatic step. Importantly, it’s activated only in the liver, not in muscle, which explains why patients with statin-related muscle symptoms often tolerate bempedoic acid well.
The CLEAR Outcomes trial (2023) showed bempedoic acid reduces cardiovascular events in statin-intolerant patients. Useful as an add-on therapy or as a primary therapy in genuine statin intolerance.
PCSK9 Inhibitors
Injectable medications (evolocumab, alirocumab) that lower LDL by 50-60%. Given fortnightly or monthly by subcutaneous injection. Reserved for patients with familial hypercholesterolaemia or very high-risk patients who can’t reach targets with conventional therapy.
The FOURIER trial (2017) and ODYSSEY-OUTCOMES (2018) established their cardiovascular benefit. In UK practice, typically accessed through specialist lipid clinics.
Inclisiran
A genuinely transformative newer option. Inclisiran is a siRNA (small interfering RNA) medication that targets PCSK9 production at the genetic level. Given as a subcutaneous injection initially, then again at 3 months, then twice yearly thereafter.
Key advantages:
- LDL reduction of 50%+ that’s sustained for 6 months between doses
- Twice-yearly dosing eliminates daily adherence challenges
- Approved by NICE (TA733, October 2021) for secondary prevention in eligible UK patients
The ORION trials (2020) established its efficacy. Inclisiran is increasingly used in NHS lipid clinics but remains under-recognised by patients and many GPs.
For patients who’ve struggled with daily statin adherence, the twice-yearly inclisiran schedule is genuinely life-changing. Two injections per year, sustained LDL reduction, no daily pill burden.
Bile Acid Sequestrants
Older medications that bind bile acids in the intestine, forcing the liver to use more cholesterol to produce replacement bile acids, which lowers blood cholesterol.
Colestyramine (Questran): The oldest agent in this class. Effective but often poorly tolerated due to gastrointestinal side effects (constipation, bloating, unpleasant powder formulation).
Colesevelam (Cholestagel): Newer agent, better tolerated. Used as an add-on to dietary measures and other lipid-lowering therapies. Particularly useful when statins are contraindicated or not fully tolerated.
Bile acid sequestrants are not first-line treatments in modern UK practice, but they have a role for patients who cannot use statins or who need additional LDL lowering beyond standard combinations. They can also be useful for managing bile acid diarrhoea in patients with that condition.
Fibrates
Fibrates (bezafibrate, fenofibrate) work differently from statins — they primarily lower triglycerides and modestly raise HDL, with smaller effects on LDL.
Important: NICE NG238 does not recommend fibrates for cardiovascular disease prevention. They are not recommended as monotherapy or in combination with statins for primary or secondary CVD prevention.
The specific role for fibrates in modern UK practice is limited to severe hypertriglyceridaemia (triglycerides >10 mmol/L), where the goal is to prevent pancreatitis rather than reduce cardiovascular events. Combining fibrates with statins increases myopathy risk and is generally avoided.
For patients with raised triglycerides in the context of overall cardiovascular risk, lifestyle modification (weight loss, alcohol reduction, glycaemic control if diabetic) and statin therapy remain the cornerstone of treatment, not fibrates.
Statin Myths, Separating Evidence From Noise
Statins are among the most discussed medications in public discourse, often inaccurately. A short evidence-based response to common concerns:
“Statins damage your muscles”
Real but uncommon. About 5-10% of patients experience muscle symptoms on statins. Most can be managed by switching statins, adjusting dose, or alternative dosing schedules. True myopathy (with elevated creatine kinase) is rare. Many patients reporting “statin muscle pain” actually have pain from other causes that coincide with statin use his is established in placebo-controlled trial data showing similar muscle complaints in placebo arms.
For patients with genuine, recurrent muscle symptoms across multiple statins, alternative agents (bempedoic acid, ezetimibe, PCSK9 inhibitors, inclisiran) provide effective options.
“Statins cause memory loss/dementia”
The FOURIER trial specifically assessed cognitive function with very low LDL levels and found no detrimental effect. Large observational studies and meta-analyses have not identified a cognitive impact attributable to statins. The original concerns appear to have been driven by selection bias and confounding rather than a genuine drug effect.
“Cholesterol isn’t really a problem”
This argument resurfaces periodically in the media and online forums. The evidence against this position is extensive: 30+ years of randomised trials, Mendelian randomisation studies (which use genetic variants to confirm causality), and consistent population-level data all confirm cholesterol — specifically LDL — as a causal cardiovascular risk factor.
The strength of evidence for cholesterol-lowering exceeds almost any other intervention in modern medicine.
“Lifestyle alone should work”
Lifestyle modification is genuinely important and should always be part of cholesterol management. Diet, weight management, exercise, and smoking cessation can meaningfully reduce cardiovascular risk. However, for patients with established disease or QRISK3 ≥10%, lifestyle alone typically doesn’t reduce LDL enough to prevent events.
Lifestyle and medication work together. Treating one as a replacement for the other usually leaves patients with suboptimal management.
“Statins are only useful if you’ve already had a heart attack”
Established by HPS (2002) and JUPITER (2008) to be incorrect. Statins benefit primary prevention patients (those without prior CVD) when cardiovascular risk is meaningfully elevated. QRISK3 ≥10% is the threshold NICE uses for considering statin therapy in primary prevention.
What Does Private Cholesterol Treatment Cost?
Realistic UK pricing for online pharmacist IP-led services:
Initial consultation: typically £30- £100. Includes review of medical history, current medications, recent blood test results, cardiovascular risk assessment, and treatment discussion.
Cholesterol blood tests: £40-£90 for a full lipid panel through private labs (Medichecks, Thriva, Randox). Often, patients already have recent NHS blood test results available.
Standard generic medications: £10-£25 per month. Atorvastatin, rosuvastatin, and ezetimibe are all generic and inexpensive.
Branded or newer medications: Varies widely. Bempedoic acid (£40-£70/month). PCSK9 inhibitors and inclisiran are typically prescribed by the NHS, even when the initial assessment is private.
Ongoing reviews: £30-£70 every 3-6 months, typically.
Annual cost (typical patient): £400-£800 total covering consultations, medications, and tests.
Private GPs and specialist consultant services cost meaningfully more. A consultation with a consultant lipidologist can be £200- £400 per appointment, with follow-ups at similar rates. Pharmacist-independent prescriber-led services sit within the more accessible price range while still providing specialist cardiometabolic depth.
The cost has to be considered against the value: structured proactive management of a condition that, if poorly managed, contributes to heart attacks, strokes, and vascular death over decades.
Who Private Cholesterol Treatment Is For
Not every patient with raised cholesterol needs private care. Honest assessment of who benefits most:
Strong fit
- Patients with statin intolerance after 2+ statin trials
- Patients not reaching NICE LDL/non-HDL targets despite full-dose statin
- Patients with raised cholesterol AND raised blood pressure AND raised blood glucose (cardio-metabolic cluster)
- Patients waiting 6-12+ months for NHS lipid clinic referral
- Patients with a family history of premature cardiovascular disease who want comprehensive risk management
- Patients wanting access to newer treatments (bempedoic acid, awareness of inclisiran)
- Busy working professionals frustrated by NHS scheduling constraints
Less appropriate fit
- Patients with straightforward, well-controlled cholesterol on a first-line statin
- Patients with suspected familial hypercholesterolaemia requiring genetic and family screening (NHS lipid clinics remain appropriate for this)
- Patients in acute distress (cardiovascular emergencies, always NHS A&E)
- Patients seeking sole care for complex multi-system disease (private cholesterol care should complement, not replace, NHS GP relationship)
The honest framing: private cholesterol treatment is a complement to NHS care, not a replacement. Most patients benefit from maintaining their NHS GP for general health, vaccinations, screening, and acute illness, while using private specialist care for structured, ongoing cardiometabolic management. The NHS doesn’t have the capacity to provide
Is private cholesterol treatment available online?
Yes. Most modern private cholesterol management is delivered through online consultations with UK-registered pharmacist independent prescribers or doctors. Blood tests are arranged through home testing kits or local phlebotomy services. Prescriptions are dispensed by partner pharmacies and delivered to the patient.
Do I need a GP referral?
No. Private cholesterol services accept self-referrals. However, sharing recent NHS blood results, current medications, and any specialist letters helps the prescriber make better-informed decisions.
Can I stay registered with my NHS GP?
Yes, and most patients should. Private specialist care for cholesterol works best alongside continuing NHS GP registration for general health needs. Your private prescriber may write to your NHS GP to inform them of your treatment, with your consent.
How long does it take to see results from cholesterol treatment?
LDL cholesterol drops within 4-6 weeks of starting an effective dose of statin. The clinical benefit (reduction in cardiovascular events) accumulates over the years. Most reviews are scheduled 6-12 weeks after starting or changing therapy to confirm response and adjust dose if needed.
Are private cholesterol medications the same as NHS medications?
Yes. Generic atorvastatin, rosuvastatin, ezetimibe, and bempedoic acid are identical regardless of whether obtained via the NHS or a private route. The difference lies in how they’re accessed, prescribed, monitored, and integrated into overall cardiometabolic management.
Can I switch back to NHS care later?
Yes. Patients can pause private care and continue cholesterol management through their NHS GP at any time. With written notes from your private prescriber, continuity with the NHS is straightforward.
What if I have familial hypercholesterolaemia?
Suspected FH requires a specialist lipid clinic referral for genetic testing and family cascade screening. NHS lipid clinics remain the appropriate primary pathway for FH. Private services can support ongoing cholesterol management once the FH diagnosis and family screening are in place through the NHS.
A Final Word On Evidence
The evidence base for cholesterol management is more robust than for almost any other intervention in modern medicine. Multiple landmark trials over 30 years, 4S (1994), HPS (2002), JUPITER (2008), IMPROVE-IT (2015), FOURIER (2017), CLEAR Outcomes (2023), consistently show that lowering LDL cholesterol reduces cardiovascular events and saves lives.
What’s changed in 2026 isn’t whether cholesterol management works. It’s how sophisticated the options have become. Twice-yearly inclisiran injections. Bempedoic acid for statin-intolerant patients. PCSK9 inhibitors for very high-risk cases. Integrated cardio-metabolic management that treats blood pressure, glucose, and cholesterol together rather than separately.
For many UK patients, NHS care effectively manages cholesterol. For patients who fall through the gaps, statin intolerance, inadequate control, complex cardio-metabolic clustering, or simply wanting more time and continuity, private specialist services exist as a complementary option.
Choosing the right pathway depends on your specific clinical picture and what matters most to you. If you’re considering private cholesterol treatment, the questions worth asking are: Have I tried the NHS pathway fully? Is my current cholesterol control optimal? Would integrated cardio-metabolic care benefit my overall risk profile? Am I willing to invest in structured private care to improve outcomes that won’t be visible for years?
For some patients, the answer is that NHS care continues to work well. For others, private cholesterol treatment fills a gap that the NHS isn’t designed to address.
About CardivaRx: CardivaRx is a specialist cardio-metabolic prescribing service launching in the UK, focused on hypertension, type 2 diabetes, and cholesterol management. Founded by a GPhC-registered pharmacist with a specialist independent prescriber qualification in cardio-metabolic conditions. Evidence-based. NICE-aligned. Online-first. Currently in development, register your interest at cardivarx.co.uk.