
Introduction
Private treatment for type 2 diabetes in the UK has changed dramatically in 2026. The NICE NG28 guideline, the UK gold standard for T2DM management, received its most significant update in over a decade in February 2026, and the prescribing landscape has shifted with it.
If you’re searching for private type 2 diabetes treatment in the UK, you’re searching at a genuinely interesting moment. SGLT2 inhibitors are now first-line for most adults. Triple therapy is the new standard for those with cardiovascular disease. GLP-1 agonists like semaglutide have become central to modern care. The conversation about T2DM is no longer just about HbA1c; it’s about cardiovascular protection, kidney protection, weight, and quality of life, all at once.
This guide covers what private T2DM treatment looks like in the UK now, how it differs from NHS care, what it costs, what the new NICE guidance actually says, and how to choose a provider who will treat you properly rather than write prescriptions.
Quick note: This is general health information, not personal medical advice. Always speak to a registered prescriber about your own treatment.
What Is Type 2 Diabetes?
Type 2 diabetes is a progressive metabolic disorder in which the body either resists the action of insulin or doesn’t produce enough of it to maintain healthy blood glucose levels. Over time, untreated or poorly controlled T2DM damages blood vessels, nerves, kidneys, eyes and the cardiovascular system.
It’s the most common form of diabetes in the UK, affecting around 4.5 million adults, with another estimated 850,000 living undiagnosed. Diabetes UK estimates an additional 5 million adults are at high risk of developing T2DM, typically those with raised fasting glucose or HbA1c in the prediabetes range.
T2DM rarely travels alone. It clusters with hypertension, raised cholesterol, central obesity and non-alcoholic fatty liver disease. This clustering, known as metabolic syndrome, is why modern T2DM care can’t be delivered in isolation from broader cardiometabolic care.
This guide focuses on type 2 diabetes in non-pregnant adults. Gestational diabetes (hyperglycaemia in pregnancy), type 1 diabetes, and other forms of diabetes (such as Maturity Onset Diabetes of the Young) are managed under different NICE guidance and are not covered here.
The clinical thresholds matter:
- HbA1c ≥48 mmol/mol (6.5%) on two occasions — diagnosis of T2DM
- HbA1c 42–47 mmol/mol (6.0–6.4%) — prediabetes / high risk
- Fasting glucose ≥7.0 mmol/L on two occasions — diagnosis of T2DM
Most adults with T2DM are diagnosed when blood is taken for another reason. The condition is largely silent until it isn’t, which is why early identification and proper treatment matter enormously.
Why People Choose Private Type 2 Diabetes Treatment in the UK
The reasons people pay for private T2DM care are remarkably consistent and frustratingly familiar to anyone who’s recently been through the NHS pathway.
1. Access to modern medication options. NHS prescribing of newer agents such as SGLT2 inhibitors and GLP-1 receptor agonists has historically been gated by Integrated Care Board (ICB) formularies, regional commissioning decisions, and stepped-care pathways, which delay access to drugs that the patient’s clinician believes are right for them. The 2026 NICE NG28 update has moved these drugs earlier in the pathway, but real-world NHS implementation lags. Private prescribing follows NICE directly, with no formulary delay.
2. Time and continuity. A 10-minute annual diabetes review at an NHS general practice, often with a different clinician each time, isn’t enough time to properly discuss medication options, side effects, lifestyle, weight management, and cardiovascular risk. Private consultations are 20–30 minutes and use the same prescriber at every visit.
3. Comprehensive cardio-metabolic care. NHS T2DM care is typically delivered by a GP, with hypertension managed in a separate appointment (often with a different GP), cholesterol in yet another, and weight via an entirely separate referral. Specialist private cardiometabolic services treat the whole picture in a single integrated plan, with a single prescriber.
4. Faster access to GLP-1s for weight management. Drugs like semaglutide (Ozempic) and tirzepatide (Mounjaro) have transformed both diabetes management and obesity treatment. NHS access is severely capacity-constrained. Private services have been the dominant route for accessing these medications in 2024–2026.
5. Convenience and continuity for working adults. Online consultations, home delivery of medication, evening and weekend appointment availability, and the same prescriber each time aren’t luxuries for working professionals with T2DM. They’re often the difference between staying engaged with care and disengaging entirely.
| Feature | NHS T2DM Care | Private T2DM Treatment UK |
|---|---|---|
| Cost to patient | Free at point of use; £9.90/item in England (or PPC) | Self-pay; £30–£250 initial consultation (depending on provider type); £15–£300+/month medication (varies by regimen) |
| Time to first appointment | Often 2–6 weeks | Usually 24–72 hours |
| Annual review length | ~10 minutes | 30 minutes |
| Continuity of the clinician | Variable | Same prescriber every visit |
| Access to SGLT2 inhibitors as first-line | Improving since Feb 2026 NICE update, ICB-dependent | Immediate, NICE-aligned |
| Access to GLP-1s | Capacity-limited, criteria-gated | Available within scope |
| HbA1c testing | Quarterly to annually | Same, often more frequent |
| CGM access | Improving for insulin users | Available across broader patient groups |
| Online delivery | Limited | Fully online services available |
| Integrated cardio-metabolic care | Fragmented across appointments | Holistic, single prescriber |
| Lifestyle and weight support | Variable, often referral-only | Built into the consultation model |
| Best for | Stable, well-controlled, and satisfied with the NHS pathway | Faster access, complex cases, those wanting modern options and integrated care |
Private care isn’t “better medicine”; most of the medication is the same. What you’re paying for is time, speed, choice, and integrated cardio-metabolic depth.
NICE NG28 (Updated 18 February 2026): What’s Actually New
The NICE NG28 update on 18 February 2026 is one of the most significant shifts in UK T2DM management in over a decade. Any private T2DM service worth paying for in 2026 will be aligned to this update. Here’s what it actually changed.
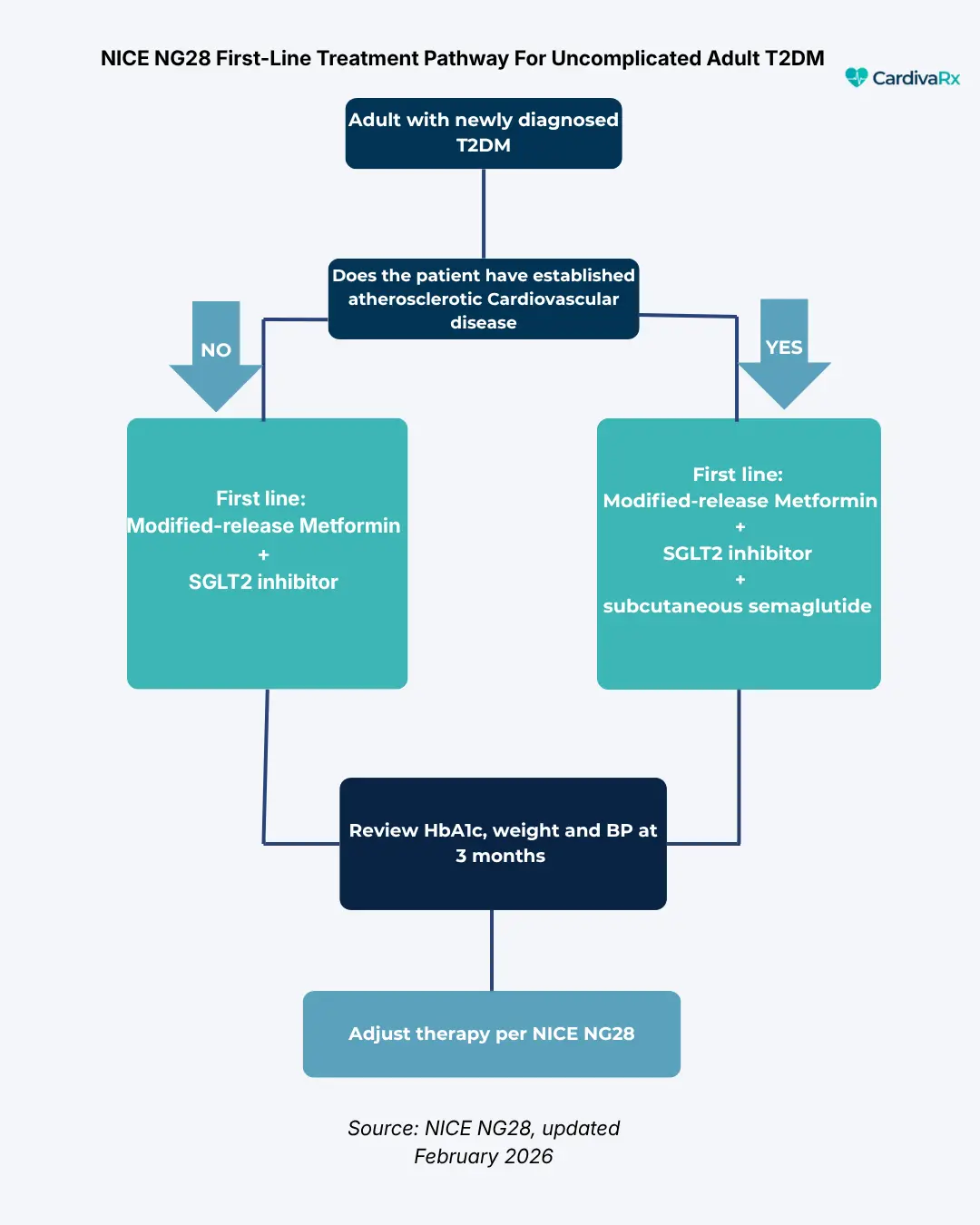
This pathway shows the first-line treatment decision for uncomplicated adult type 2 diabetes per NICE NG28 (February 2026 update). The full guideline includes additional considerations for patients with heart failure, chronic kidney disease, frailty, and complex multi-morbidity. See the full NICE NG28 guideline for these scenarios.
1. SGLT2 Inhibitors Are Now First-Line For Most Adults
Previously, SGLT2 inhibitors (empagliflozin, dapagliflozin, ertugliflozin, canagliflozin) were typically added as second-line therapy after metformin. The February 2026 update moves them up: metformin plus an SGLT2 inhibitor is now the standard first-line dual therapy for most adults with T2DM, regardless of whether they have established cardiovascular disease.
Why: large outcome trials have demonstrated that SGLT2 inhibitors do far more than lower glucose. They reduce cardiovascular events, slow chronic kidney disease progression, reduce hospitalisation for heart failure, and modestly reduce body weight. NICE concluded the evidence is now strong enough to make them first-line.
To understand the depth of the evidence: until 2015, diabetes drugs were judged mainly by HbA1c reduction. EMPA-REG OUTCOME changed everything by showing empagliflozin reduced cardiovascular death by 38%, independent of glucose lowering. Subsequent trials DAPA-HF, EMPEROR-Reduced, EMPEROR-Preserved, CREDENCE, DAPA-CKD, EMPA-KIDNEY established SGLT2 inhibitors as cardioprotective AND renoprotective across the spectrum of cardiovascular and kidney disease, with benefits often independent of diabetes status
2. Triple Therapy First-Line For Established Cardiovascular Disease
For adults with T2DM and existing atherosclerotic cardiovascular disease, the update goes further: metformin + SGLT2 inhibitor + subcutaneous semaglutide is now standard first-line therapy. This is a substantial intensification compared to the previous “metformin first, escalate if needed” pathway.
The rationale: in this high-risk group, waiting for HbA1c to drift up before adding cardiovascular-protective agents costs lives. Modern cardiovascular outcome trials of GLP-1 agonists have demonstrated meaningful reductions in major adverse cardiovascular events.
3. Modified-Release Metformin Preferred
The update recommends modified-release metformin as the standard first-line formulation, with patients currently tolerating standard-release able to continue. The rationale is improved gastrointestinal tolerability and adherence to small changes that compound over years of treatment.
4. Tighter Blood Pressure Targets
For adults with T2DM, NICE now recommends a general BP target of below 130/80 mmHg, tighter than the general adult target of 140/90 in NG136. For those at especially high cardiovascular or kidney risk, a systolic pressure below 120 mmHg is encouraged. Older or frail adults may have a relaxed target of below 140/90.
This is where T2DM care can’t be separated from hypertension care, exactly the integrated cardio-metabolic approach specialist services are built around.
5. Continuous Glucose Monitoring Expanded
CGM is now recommended at diabetes onset for anyone on insulin, on agents that can cause hypoglycaemia, or where CGM aids management. NHS availability lags this. Private services can offer broader access to CGM.
6. Individualised Glycaemic Targets
Less prescriptive HbA1c targets, greater emphasis on shared decision-making, and recognition that the “right” HbA1c depends on age, comorbidities, hypoglycaemia risk, and patient preference. A tight HbA1c of 48 mmol/mol may be ideal for a fit 50-year-old, but it is the wrong target for an 80-year-old with frailty.
7. Sick Day Rules Strengthened
Clearer guidance on which medications to pause during acute illness (especially SGLT2 inhibitors due to euglycaemic DKA risk and metformin due to lactic acidosis risk if dehydrated), and structured guidance on restarting therapy after recovery.
How Private Type 2 Diabetes Treatment Works in the UK: Step by Step
A reputable private T2DM service should follow a clear, NICE NG28-aligned pathway. Here’s what you should expect.
A note on physical examinations: While most modern T2DM care can be delivered online including consultation, prescribing, monitoring, and lifestyle support certain components require in-person assessment. Annual diabetic foot examination, retinal screening, and (occasionally) injection technique training are typically best handled either through your NHS GP (often free), through partner physical clinics, or through patient self-monitoring with structured guidance. A reputable online private T2DM service will have clear pathways for ensuring these physical components are covered, even if they aren’t delivered in-house
Step 1: Initial Consultation
Whether in person or via secure video, your first appointment covers your full medical history, family history, current medications, lifestyle, current HbA1c, any symptoms, and, crucially, your goals for weight, glycaemic control, medication preferences, cardiovascular risk reduction, or all of these together.
Step 2: Baseline Investigations
Before treatment initiation or major change, NICE recommends:
- HbA1c (current and ideally a 6-12 month trend)
- Renal function (eGFR, urine albumin: creatinine ratio)
- Lipid profile
- Liver function (especially given the prevalence of Non-Alcoholic Fatty Liver Disease in T2DM)
- Blood pressure assessment (often via ABPM or HBPM in cardio-metabolic clinics)
- 10-year cardiovascular risk score (QRISK3)
- Body composition (weight, BMI, waist circumference)
- Foot examination
- Retinal screening status
Some of these can be ordered through the private service; others require coordination with your NHS GP or independent labs.
Step 3: Treatment Plan
Following the February 2026 NICE update, the typical first-line plan is:
- No cardiovascular disease, no kidney disease, no heart failure: modified-release metformin + an SGLT2 inhibitor
- Established atherosclerotic cardiovascular disease: modified-release metformin + SGLT2 inhibitor + semaglutide (subcutaneous)
- Heart failure or chronic kidney disease: SGLT2 inhibitor anchored therapy, with metformin and other agents added or sequenced based on tolerability and renal function
A good private prescriber will explain which combination is right for you and why, what the realistic timeline for an HbA1c response looks like (typically 3–6 months), and what the side-effect profile of each agent is.
Step 4: Lifestyle and Weight Management
NICE NG28 explicitly anchors pharmacological therapy on a foundation of dietary and lifestyle interventions. The 2026 update now cross-references NICE’s guideline on the management of overweight and obesity, recognising that for many adults with T2DM, sustained weight loss is the most powerful single intervention.
Evidence-based lifestyle changes that genuinely move HbA1c:
- Sustained 10–15% weight loss can induce T2DM remission in a meaningful subset of patients, particularly within 6 years of diagnosis
- Mediterranean or DASH-style eating patterns robustly affect HbA1c, BP and lipid effects
- Resistance training plus aerobic activity improves insulin sensitivity
- Sleep optimisation: Sleep deprivation worsens insulin resistance
- Alcohol moderation is particularly important for those on insulin or sulfonylureas
- Smoking cessation is non-negotiable; smoking dramatically increases the cardiovascular risk of T2DM
A serious private prescriber will spend genuine time on these rather than skip past them to write a prescription.
Step 5: Ongoing Review
T2DM is a progressive condition. Treatment is rarely set and forget. A typical private review schedule:
- 3 months after starting or changing medication: check tolerability, repeat HbA1c, review side effects, repeat renal function if on SGLT2i or RAAS-blocker
- 6 months: HbA1c, weight, BP review, dose adjustment
- Annually: full cardio-metabolic review, retinal screening status check, foot review, lipid review, renal function
If your private service doesn’t structure follow-up like this, that’s a red flag.
Who Can Provide Private Type 2 Diabetes Treatment in the UK?
Four main categories of clinicians you’ll encounter:
Private GPs. Generalists, CQC-registered, treating T2DM as part of broader primary care. Initial consultation typically £150–£250. Best for those wanting general care with T2DM as one component.
Consultant diabetologists/endocrinologists. Specialists, GMC-registered, based in private hospitals (HCA, Spire, Cleveland Clinic London, Harley Street). Initial consultation typically £300–£450+. Best for complex T2DM, type 1 diabetes, MODY, secondary diabetes, or where there’s diagnostic uncertainty.
Pharmacist Independent Prescribers (IPs). GPhC-registered pharmacists with the IP qualification are increasingly the backbone of private prescribing for chronic diseases in the UK. They tend to specialise (cardio-metabolic, women’s health, weight, mental health) and typically offer the lowest price point with the longest consultation time per pound spent.
Other Independent Prescribers. Nurse and paramedic IPs also operate in this space, though their prescribing role for T2DM is more limited.
For uncomplicated adult T2DM, a pharmacist IP working within a cardio-metabolic scope, or a private GP working to NICE NG28, will deliver the same clinical outcome as a diabetologist at a fraction of the cost. Referral to a diabetologist is appropriate where there’s diagnostic uncertainty, complex secondary causes, severe insulin resistance, advanced complications, or coexisting endocrine conditions.
| Component | Typical Private Cost (UK) |
|---|---|
| Initial consultation (private GP) | £150–£250 |
| Initial consultation (diabetologist) | £300–£450+ |
| initial consultation (pharmacist IP, online) | £30–£120 |
| Cardio-metabolic blood panel (HbA1c, U&Es, lipids, LFTs, ACR) | £100–£350 |
| ABPM | £125–£550 |
| Retinal screening | £100–£300 |
| Follow-up consultation | £40–£200 |
| metformin (generic) – monthly cost | £5–£15 |
| SGLT2 inhibitor – (monthly cost) | £30–£50 |
| GLP-1 (semaglutide) – (monthly cost) | £150–£300 |
| tirzepatide (Mounjaro) – (monthly cost) | £180–£350 |
Note on retinal screening: The NHS Diabetic Eye Screening Programme (DESP) provides annual or biennial retinal screening free of charge to all UK adults diagnosed with diabetes from age 12. Most patients receive this through their NHS GP referral. Private retinal screening offers advanced imaging (OCT, ultrawidefield) and faster turnaround for patients who want a more comprehensive assessment, but isn’t routinely needed where NHS DESP is accessible.
This:
- Adds clinical credibility (you’re not trying to sell something patients can get free)
- Aligns with NICE NG28 (which assumes NHS DESP access)
- Protects you regulatorily — never suggest paying for something the NHS provides routinely
- Sounds clinically grounded, not marketing-driven
Where the meaningful savings are: Online pharmacist-IP-led services typically bundle consultation, prescription, and dispensing into a single transparent monthly fee. The headline cost gap with hospital-based diabetology pathways is substantial, especially when ongoing care over years is factored in.
The cheaper route isn’t automatically the right one, but for uncomplicated, NICE-aligned T2DM care, it usually is.
Modern T2DM Medications: A Quick Tour
The medications most likely to feature in your treatment plan, in plain English:
Metformin (modified-release preferred in 2026). First-line foundation drug. Reduces liver glucose production and improves insulin sensitivity. Modest weight benefit. Watch for GI upset (improved on MR formulation) and vitamin B12 deficiency on long-term use.
SGLT2 inhibitors (empagliflozin, dapagliflozin, ertugliflozin, canagliflozin). Now first-line alongside metformin for most adults. Work by increasing glucose excretion via the urine. Major benefits: cardiovascular and kidney protection, modest weight loss, and reduced risk of heart failure hospitalisation. Watch for genitourinary infections and the rare but serious euglycaemic DKA, particularly during acute illness.
GLP-1 receptor agonists (semaglutide, tirzepatide, dulaglutide, liraglutide). Now first-line for T2DM with established cardiovascular disease, and increasingly used for weight management within obesity care. Slow gastric emptying, increased satiety, and improved glycaemic control. Substantial weight loss. Watch for GI side effects (especially on initiation and dose escalation), and contraindicated in those with personal or family history of medullary thyroid cancer or MEN2.
DPP-4 inhibitors (sitagliptin, linagliptin, alogliptin). Modest HbA1c effect, weight-neutral, generally well tolerated. Less prominent in the 2026 NICE pathway than they once were, but still useful in older patients or where other agents aren’t tolerated.
Sulfonylureas (gliclazide). Older class. Effective at lowering HbA1c but causes weight gain and hypoglycaemia. Used less first-line in 2026 but still relevant in specific contexts.
Insulin. The eventual treatment for many people with T2DM is particularly important as the condition progresses. Modern long-acting analogues (insulin glargine, degludec) are simpler to use than older insulins. Initiating insulin in T2DM requires structured education and support, not something to be done casually.
How to Choose a Private Type 2 Diabetes Service in the UK
Ten things to check before paying anything:
Ten things to check before paying anything:
- Is the prescriber registered? GPhC for pharmacists, GMC for doctors, NMC for nurses. Public registers, free to search.
- Is the service CQC-registered (if England) or equivalent?
- Is the service NICE NG28-aligned, specifically reflecting the February 2026 update? If they’re still working from pre-2026 pathways, walk away.
- Is the consultation at least 20 minutes, with follow-up baked in (not charged ad hoc)?
- Are appropriate baseline investigations ordered before starting or changing therapy?
- Is there a clear plan for cardio-metabolic risk factors (BP, cholesterol, weight), not just glucose?
- Is pricing transparent — total annual cost, including medication, not just the headline consultation fee?
- Do you see the same prescriber at every review?
- What’s the policy if you have side effects out of hours?
- Are reviews independent? Trustpilot and Google reviews tell you more than testimonials on the company’s own site.
Any provider unwilling to answer those plainly is not the right provider.
CardivaRx: Specialist Cardio-Metabolic Care for T2DM (Coming soon)
CardivaRx is being built specifically to address this gap: a UK private cardio-metabolic prescribing service, led by a GPhC-registered pharmacist and Independent Prescriber, treating type 2 diabetes alongside hypertension and raised cholesterol as one integrated cardio-metabolic picture rather than three separate conditions. For detailed information on cholesterol treatment options, read our complete guide to private cholesterol treatment in the UK.
The model is online-first, fully aligned to NICE NG28 (including the February 2026 update), with structured diagnostic workup, baseline cardio-metabolic blood panels, longer consultations, and continuity of prescriber.
We’re pre-launch while the Independent Prescribing qualification is finalised. Still, you can register your interest now to be first in line when the service opens, and to be the first to receive new evidence-based guides like this one.
Type 2 Diabetes and Men’s Hormonal Health: An Often-Missed Connection
This is a clinical relationship that deserves more attention than it gets in routine T2DM care.
There is a well-established bidirectional clinical association between type 2 diabetes and low testosterone in men. Men with T2DM have a substantially higher prevalence of biochemical hypogonadism compared to men without diabetes. Insulin resistance, visceral adiposity, sleep apnoea, and chronic inflammation all contribute. Low testosterone, in turn, worsens insulin sensitivity and central adiposity, creating a self-reinforcing cycle.
The clinical evidence (Bhasin et al., HIM Study, T-Trials) supports active investigation of testosterone status in men with T2DM who have symptoms of hypogonadism, fatigue, low libido, erectile dysfunction, loss of morning erections, reduced muscle mass, and depressed mood.
Whether testosterone replacement therapy is appropriate in any given man with T2DM and low T is a complex clinical decision. It requires careful biochemical confirmation (multiple morning total T measurements, free T calculation, LH/FSH, SHBG, PSA, full blood count), thorough exclusion of contraindications, and ongoing structured monitoring.
What’s clear is that the conversation should happen. A specialist cardio-metabolic service will assess and address the whole metabolic-hormonal picture in men, not just glucose.
CardivaRx’s cardio-metabolic scope is currently focused on hypertension, type 2 diabetes and dyslipidaemia. Men’s hormonal health is a clinically intertwined area that we will expand into in the medium term as our prescribing experience and governance infrastructure mature. If this is relevant to you, register your interest to be notified of the expanded scope.
Frequently Asked Questions
Can I get private type 2 diabetes treatment without seeing my NHS GP first?
Yes. You don’t need a GP referral to access private T2DM treatment in the UK. A reputable private service will take a full history, request appropriate tests, and independently initiate or modify treatment, with your consent, and share the outcome with your NHS GP for joined-up care.
Is online private T2DM treatment safe?
When delivered by a registered prescriber with proper diagnostic workup, baseline bloods, structured follow-up and clear safeguarding pathways, online T2DM treatment is as clinically safe as in-person care for the majority of adults with uncomplicated T2DM. Complex cases, type 1 diabetes, advanced complications, or insulin initiation usually warrant at least some in-person specialist input.
Will my private T2DM treatment cost less than NHS care?
For people who don’t pay for NHS prescriptions (over-60s, exempt groups, or those with a Prescription Prepayment Certificate), NHS care is essentially free. For everyone paying the full NHS prescription charge, modern T2DM treatment combinations (metformin + SGLT2i + GLP-1) can add up quickly. Some private services with bundled monthly subscription pricing work out competitively overall, especially when consultation time and continuity are factored in.
Can a pharmacist prescribe diabetes medication in the UK?
Yes, if they hold the Independent Prescribing qualification annotated on their GPhC register entry and prescribe within their declared scope of practice. T2DM, hypertension and dyslipidaemia are recognised IP scopes within cardio-metabolic specialism.
Will my private service follow NICE NG28?
A reputable one will, including the February 2026 update. Ask explicitly. Services that still work with pre-2026 pathways are clinically out of date.
What about GLP-1s for weight loss?
This is a complex area. GLP-1 receptor agonists like semaglutide (Wegovy for obesity, Ozempic for diabetes) and tirzepatide (Mounjaro) are licensed in the UK for specific indications. Private prescribing of these medications has driven a major market shift in 2024–2026. However, they’re not appropriate for everyone, side effects can be significant, and ongoing monitoring is essential. We’ll cover GLP-1s in detail in a dedicated guide.
What’s the difference between a private GP and a pharmacist prescriber for T2DM?
A private GP treats T2DM as part of broader primary care. A pharmacist Independent Prescriber operating within a cardiometabolic scope focuses specifically on conditions such as T2DM, hypertension, and dyslipidaemia. Both work to NICE NG28. Pharmacist IP services typically cost less and offer longer consultation time per pound spent; private GPs are better suited to multi-system or undifferentiated symptoms.
How quickly can I start treatment privately?
For uncomplicated T2DM, you can complete the initial consultation within 24–72 hours and start treatment within 1–2 weeks, assuming baseline investigations are clear. Anyone offering same-day prescriptions for new T2DM therapy without a baseline assessment is cutting clinical corners.
Can private services prescribe insulin?
Some can, within scope. Insulin initiation requires structured education, blood glucose monitoring infrastructure, hypoglycaemia awareness training, and clear escalation pathways. Not all private prescribers offer this, and it’s typically reserved for established services with mature governance.
Final Thoughts
Private type 2 diabetes treatment in the UK is in a genuinely different position in 2026 than it was even two years ago. The February 2026 NICE NG28 update has substantially shifted the prescribing landscape. The conversation has moved beyond just lowering HbA1c; modern T2DM care is about cardiovascular protection, kidney protection, weight management, and quality of life, all together.
For many UK adults with T2DM, private specialist care is no longer about getting “better medicine” — most of the medication is the same. It’s about getting the right medicine faster, with proper consultation time, from a prescriber who understands cardiometabolic risk as a whole and who’ll still be the same prescriber at next year’s review.
If you’d like to be among the first to access CardivaRx when we launch, register your interest here. And if you want to understand how private hypertension treatment works alongside diabetes care, our complete guide to private hypertension treatment in the UK is the companion read.
References
- Lean MEJ et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT). The Lancet.
- NICE. Type 2 diabetes in adults: management (NG28). Last updated 18 February 2026. https://www.nice.org.uk/guidance/ng28
- NICE. Hypertension in adults: diagnosis and management (NG136). Last updated 26 February 2026.
- Diabetes UK. Diabetes statistics.
- NHS. Type 2 diabetes overview. https://www.nhs.uk/conditions/type-2-diabetes/
Disclaimer
This article is general health information and does not constitute personal medical advice. CardivaRx is in pre-launch as the founder completes the Independent Prescribing qualification. No prescribing services are currently being offered. Always consult a registered healthcare professional about your own treatment.